

Introduction
Say the word "sociology" out loud. Right now.
If your "S" or "C" came out clean, the rest of this article is for someone else. But if it came out as "sothiology" or "tothiology", or with a wet, slushy edge, you have an S lisp, and you're in the right place.
What is an S Lisp?
An S lisp is the most common articulation error and the most fixable one. If you would do 15 minutes of focused practice a day, you would see a clean "S" within 6-12 weeks, without surgery, without anyone knowing you are working on it.
The American Speech-Language-Hearing Association classifies sibilant errors as among the most responsive to targeted practice in teens and adults.
The problem is not "fixing a lisp is difficult," but the problem is that almost everything written about it sums up to two different lisps together and provides you with exercises that work for one and not the other.
This blog separates them first, so you can fix them. Read more about how.
The Groove Test: Which lisp do you have?
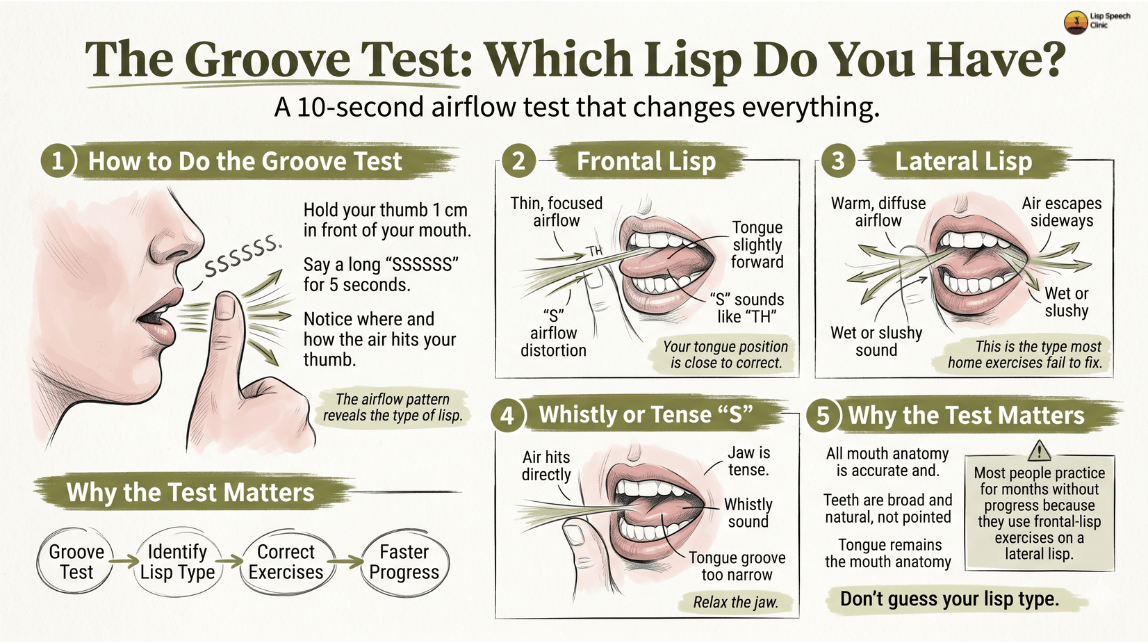
Speech infographic for identifying lisp types through airflow patterns.
You need to know which type of "S" lisp you have before practicing anything.
Hold your thumb about 1 cm in front of your mouth. Say a long "ssssssssss" for 5 seconds. Pay attention to where you feel the air.
- If the air hits your thumb straight on, in a thin, cold stream: Your tongue position is close to correct. You may have a mild frontal lisp (tongue too far forward, "s" sounds like "th").
- If the air spills out the sides of your mouth, warm and diffuse: you have a lateral lisp. The "s" sounds wet or slushy. This is the one most home programs fail to fix because they don't address the airflow problem.
- If the air hits your finger, but the sound is whistly or tense: your tongue groove is too narrow. Same exercises as frontal, but relax your jaw.
That ten-second test is the Groove Test, and it determines everything that follows. If you have a frontal lisp, Step 1 will likely solve it within weeks. If you have a lateral lisp, Step 1 alone will not work; you need the airflow fix in Step 2 first.
Most people who practice for months without progress are doing frontal-lisp exercises on a lateral lisp. Don't be them.
The Groove Test told you what type of lisp you have. The 2-minute lisp test tells you how severe it is, which exercises to start with, and how long your specific case will likely take.
Find out exactly which lisp you have
Our free assessment runs spectral audio analysis on your speech and tells you which lisp pattern shows up — so you start at the right place instead of guessing.
Take the Free Lisp Assessment →Why the S sound breaks so easily
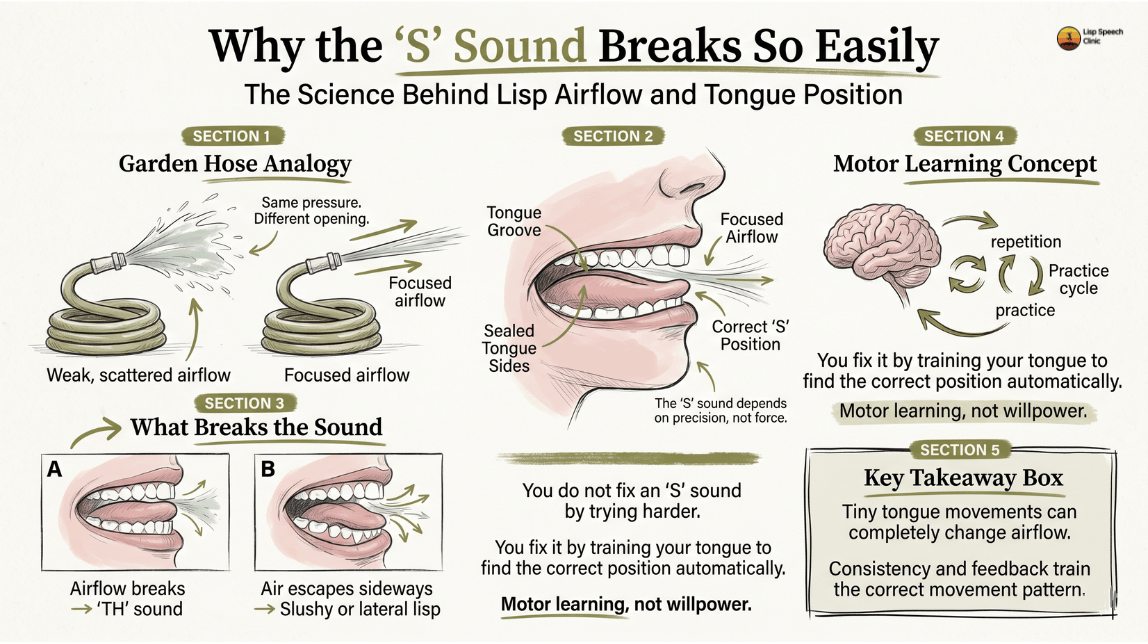
Speech infographic on airflow, tongue placement, and motor learning for correct “S” pronunciation.
Think of your tongue as a garden hose.
When you put your thumb over the end of a hose, water sprays in a wide, weak stream. When you press the opening into a thin slit, water shoots out fast and focused. Same water pressure, completely different result.
The "s" sound is the focused jet. Your tongue creates a narrow groove down its center, your tongue sides press against your upper back teeth to seal the edges, and air shoots through the groove in a tight stream toward your front teeth.
Move the tongue 2mm forward, and it touches the teeth. The jet becomes "th." Drop one side of the seal, and air leaks out laterally, the jet becomes a slushy spray.
You cannot make a particular sound by trying harder. You produce it by training your tongue to find the correct position automatically.
That is a motor learning problem, not a willpower problem. Motor learning works well with repetition and feedback, not intensity.
Step 1: Find the position
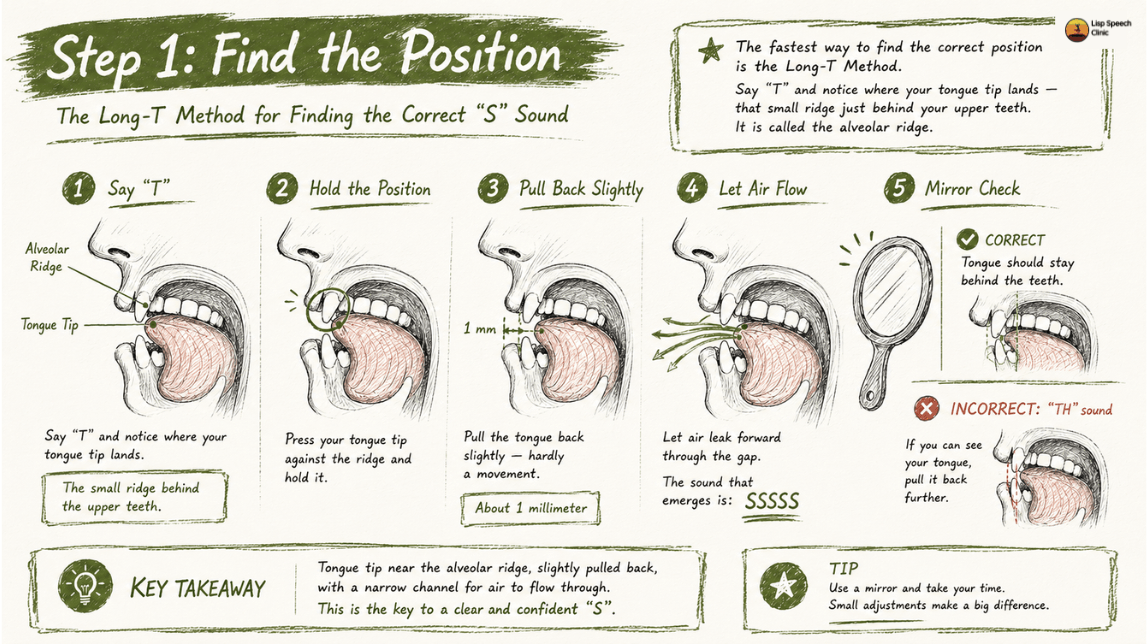
Lisp type identification infographic based on airflow and tongue position.
The fastest way to find the correct tongue position is the long-T method.
Say "tea." Notice where your tongue tip lands, that small ridge just behind your molars. It is called the alveolar ridge.
Now:
- Press your tongue tip against the molars as if to say "t."
- Hold it. Do not release.
- Pull the tip back about one millimeter. (hardly a movement)
- Let air leak forward through the gap you just created.
The sound that emerges is "ssssss." Use a mirror. Your tongue should not be visible between your teeth. If you can see it, you're making "th" — pull it back further.
If the long-T method doesn't click after ten tries, try the butterfly position.
Smile a little, notice how the sides of your tongue are pressing firmly against your upper molars (you should feel the back teeth touching the tongue's edges) and blow air to the middle. This works better for people whose tongues rest low in the mouth.
One of the two will work for you within five minutes.
Mark, which one is your position from now on?
Step 2: Hold the position
Finding the position once is easy. Holding it for ten seconds without it falling apart is tricky and a skill.
Hold the "ssssss" for ten full seconds. Use the Groove Test from earlier: place your finger one cm from your mouth and feel the airflow. If the air is still spilling sideways at second eight, your tongue is tiring, and the seal is breaking before the sound stabilizes itself.
This is how lateral lisps get fixed, and most people quit.
Use the straw technique: place a pen between your teeth, lengthwise, with the tip just behind your front teeth. Direct your airflow along the straw.
Practice holding the "s" through the pen for thirty seconds at a time. The pen forces air down the center because there's nowhere else for it to go. After two weeks, your tongue learns the channel even without the straw. Voila!
Two minutes, twice a day. That's it for week one.
Boring, I know, but it's necessary.
Motor learning study published in the Journal of Speech, Language, and Hearing Research consistently finds that high-frequency, low-variability practice produces faster acquisition than longer sessions of mixed practice.
Your tongue needs repetition.
Not sure which exercises fit your lisp type?
Our 2-minute assessment uses guided audio prompts to identify whether your lisp is frontal, lateral, or mixed and gives you a tailored plan built for that specific pattern.
Take the assessment →Step 3: Stack it into words
The hardest part of fixing a lisp is not finding the position. It's keeping the position when your brain is busy thinking about a word.
Practice in this order. Ten repetitions of each before moving to the next category. Do not skip stages.
Interactive Audio Guide
S at start (easiest)
S at end (medium)
S blends (hardest)
Sentences:
For each sentence, do three reps.
First rep: exaggerate every "s" until it almost whistles.
Second rep: Take it back to normal.
Third rep: Amp up the speed as if you are conversing.
If the third rep collapses back into a lisp, it's ok, slow down and repeat the cycle once again.
The method teaches your tongue what "too far in the right direction" feels like, which makes "correct" easier to find at speed.
Keep the momentum of this stage for at least two weeks.
Most people rush past it because the words feel easy in isolation. Then they get into a conversation, and the old pattern wins.
The point of stage three isn't to learn the words; it's to make the new tongue position survive the cognitive load of word retrieval.
Simply put, the brain needs to learn the correct tongue pattern.
Step 4: Carry it into speech
This stage feels like a tortoise winning the rabbit race because it is slow. That's how motor habits get rewritten.
Pick one conversation per day to monitor. Not every conversation. Not every word. Just S sounds, in one conversation.
Trying to monitor everything is the most common reason people abandon Lisp work.
Your working memory cannot run a speech-monitoring loop and a normal conversation simultaneously for long.
Read aloud for ten minutes daily a book, a news article, a Reddit thread, anything with continuous text. Your brain needs to hear your corrected voice in flowing speech, not just in drills.
Record yourself once a week. Two minutes, talking about literally anything: what breakfast you ate, which movie you watched, or about your day. Listen back.
The slips will accumulate around specific patterns: fast speech, certain blends, words you say often. Those clusters become the next week's drill targets.
This loop record, identify, target, drill is the entire game from week six onward.
What the research actually says
Three findings change how you should practice.
Feedback beats effort. A 2016 randomized trial by McAllister, Byun, and Campbell, published in Frontiers in Human Neuroscience, found that visual-acoustic biofeedback produced significantly faster acquisition of /s/ and /r/ sounds than traditional articulation therapy alone. Translation: a mirror, a recording, or an app showing you what your sound looks like will outperform any amount of unfocused practice. Use feedback every session.
Frequency beats duration. A systematic review by Lousada and colleagues (2013) in the International Journal of Language & Communication Disorders found that short, frequent practice sessions produce faster motor learning than longer, less frequent ones. Twenty minutes a day across two sessions outperforms sixty minutes once.
Most cases resolve. Population data from Wren et al. (2016), published in the Journal of Speech, Language, and Hearing Research, tracked over 7,000 children and found persistent sibilant errors in roughly 3.6% of eight-year-olds — meaning the majority resolve, with or without therapy, when practice happens. The 3.6% that persist into adulthood are the population this guide is written for, and the same techniques work they just take longer.
If you have practiced consistently for eight weeks with no measurable change, stop and see a speech-language pathologist. The block is usually structural, undiagnosed tongue-tie, dental alignment, or high-frequency hearing loss in the range where "s" lives (4,000–8,000 Hz).
One last thing
If you're an adult reading this, you've probably had your lisp for fifteen years or more. You've avoided selected words. You've cringed at your voicemails. You've watched and listened to yourself in videos and looked away.
Six weeks. That's the timeline most adults need to fix what's been there for decades. The technique isn't new.
What's new is having a way to do it privately, with feedback that's actually accurate, without booking sessions or saying the word "lisp" out loud to anyone.
That's why Top Speech Health is launching Lisp Speech Program. The protocol from this article, built into a program that listens to every "s" you make and tells you what to fix.
Fifteen minutes a day. In your home. No appointments. No witnesses.
You've waited long enough.
Sign up to reserve early access when the Lisp Speech Clinic launches.
FAQs
Most adults see clear improvement within six to twelve weeks of daily 15–20 minute practice. Full carryover into spontaneous conversation typically takes three to six months. Children progress faster because their motor patterns are less ingrained. Lateral lisps take longer than frontal lisps because the airflow correction is harder to self-monitor.
For frontal lisps and many mild lateral lisps, yes — a structured home program with feedback (mirror, recording, or app) works for the majority of cases. Severe lateral lisps, lisps with no visible improvement after eight weeks, and lisps with suspected structural causes (tongue-tie, dental issues) need professional assessment.
Try the butterfly position from Step 1: smile slightly, press the sides of your tongue against your upper molars, and blow down the center. If neither method produces a clean "s" within a week, the Groove Test likely showed lateral airflow — go straight to the straw technique in Step 2 before returning to placement work.
Mechanically they are the same error — "s" and "z" use identical tongue positions. The only difference is that "z" is voiced (vocal cords vibrate) and "s" is voiceless. Per ASHA, fixing one almost always fixes the other. Practice "s" first, then add voice for "z."
Frontal lisps are developmentally normal until age 4½ and many resolve on their own. After age 5, frontal lisps should be evaluated. Lateral lisps are never developmental — they should be evaluated as soon as they're noticed, regardless of age, because they don't self-correct.
Sources
American Speech-Language-Hearing Association. Speech Sound Disorders: Articulation and Phonology (Practice Portal).
Establishes diagnostic criteria, age norms, and evidence-based treatment frameworks for sibilant errors.
View SourceMcAllister Byun, T., & Campbell, H. (2016). Differential effects of visual-acoustic biofeedback intervention for residual speech errors. Frontiers in Human Neuroscience, 10:567.
Found biofeedback produced significantly faster sound acquisition than traditional therapy.
View SourceWren, Y., Miller, L. L., Peters, T. J., Emond, A., & Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old. Journal of Speech, Language, and Hearing Research, 59(4).
Found persistent sibilant errors in approximately 3.6% of children at age 8.
View SourceLousada, M., et al. (2013). Phonological and articulation treatment approaches in Portuguese children with speech sound disorders: A randomised and controlled study. International Journal of Language & Communication Disorders, 48(2).
Demonstrated structured articulation drills produce significant gains; supports frequent short sessions.
View SourcePreston, J. L., Brick, N., & Landi, N. (2013). Ultrasound biofeedback treatment for persisting childhood apraxia of speech. American Journal of Speech-Language Pathology, 22(4).
Showed visual feedback accelerates acquisition of difficult sounds including /s/.
View SourceShriberg, L. D., Tomblin, J. B., & McSweeny, J. L. (1999). Prevalence of speech delay in 6-year-old children and comorbidity with language impairment. Journal of Speech, Language, and Hearing Research, 42(6).
Foundational dataset still cited in current ASHA guidelines.
View SourceMayo Clinic. Speech disorders: Symptoms and causes.
Accessible overview of articulation disorders.
View SourceNational Health Service (UK). Speech and language therapy.
Public guidance on accessing articulation therapy.
View Source